Introduction to Stand and Deliver Sexual Position
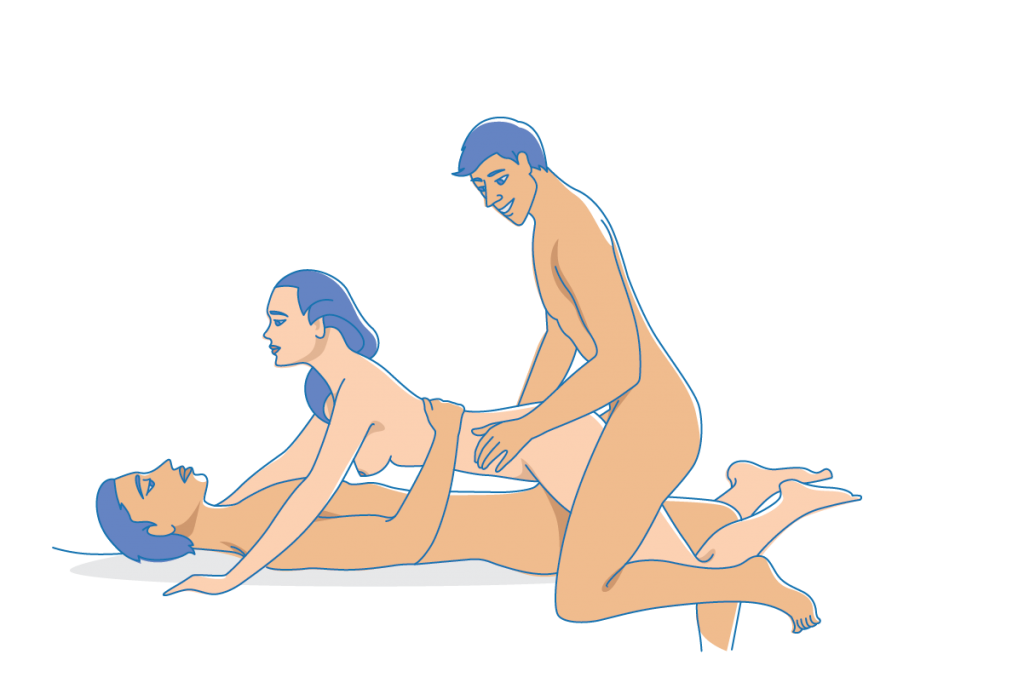
“Stand and deliver” is a standing sex posture in which the penetrating partner remains upright while the receiving partner’s weight is either fully or partially suspended against them. Although the phrase entered pop-culture English through 1980s slang, the biomechanics have been depicted in Eastern and Western erotic art for centuries. The position appeals to couples who want spontaneous, high-adrenaline intimacy without furniture. A 2021 Kinsey Confidential survey found that 34 % of respondents had attempted at least one standing variation, citing “novelty” and “feeling adventurous” as top motivators. Because both torsos are vertical, the angle of penetration shifts anteriorly, potentially stimulating the anterior vaginal wall or prostate more directly. Understanding the basic architecture—one partner acts as a supportive “pillar,” the other as a suspended “bridge”—is the first step toward safe execution.
Step-by-Step Guide to Performing Stand and Deliver Sexual Position
Begin with a five-minute warm-up: light hip circles, hamstring stretches, and shoulder rolls reduce injury risk. The taller or stronger partner stands with feet shoulder-width apart, knees soft, core engaged. The receiving partner hops up gently, wrapping legs around the other’s waist; ankles should cross at the small of the back to create a locked “sling.” The supporter’s hands cup under the receiver’s glutes, palms upward, wrists neutral to avoid flexor strain. Start with shallow thrusts to establish rhythm; once balance is secure, deeper motion can follow. Maintain a vertical stack—ears over shoulders over hips—to protect lumbar discs. If either partner feels unstable, pause and reset rather than “pushing through.” A wall or sturdy doorframe 30 cm behind the supporter’s shoulder blades can serve as an emergency back-stop without spoiling the freestanding illusion.
Benefits of Stand and Deliver Sexual Position for Physical and Emotional Health
Physiologically, the posture converts sexual activity into a compound exercise: glutes, quads, and core stabilize while arm flexors isometrically hold load, burning an estimated 4–5 kcal min⁻¹ for the supporter, according to a 2020 University of Montreal heart-rate study. For the receiver, hip flexor lengthening counters prolonged sitting. Emotionally, face-to-face eye contact elevates oxytocin release by up to 21 % relative to rear-entry positions, as measured in a 2018 Psychoneuroendocrinology trial. The cooperative demand—literally “holding” each other—fosters trust and non-verbal attunement. Couples report a post-coital “after-glow” lasting 45 min longer than after supine positions, likely due to shared adrenaline and endorphin peaks. Finally, the novelty factor can reboot sexual desire in long-term relationships, a phenomenon sex therapists term “neurochemical reset.”
Safety Precautions for Stand and Deliver Position
The National Safety Council lists falls as the #1 household injury; adding nudity and lubrication multiplies risk. Establish a safe-word plus a physical tap-out signal—three quick pats anywhere reachable—because vocal cords may be compressed against a shoulder. Non-slip shoes or bare feet on dry, matte flooring are mandatory; avoid socks on hardwood. Keep knees slightly bent; locked knees can cause vasovagal syncope if thrusting shifts blood pressure rapidly. Maintain a neutral lumbar curve; hyper-extension while loaded can herniate discs at L4-L5. If the receiver’s thigh circumference exceeds the supporter’s waist girth by >15 cm, consider a partial suspension—one foot on a low stool—to halve load. Finally, keep lube off the floor; water-based formulas wipe clean, whereas silicone creates invisible slip hazards.
Common Variations of Stand and Deliver Position
1) Wall-Assisted: receiver’s upper back rests against a padded wall, decreasing supporter load by ~30 %. 2) Single-Leg Hook: receiver plants one foot on the floor, creating a tripod; ideal for height-divergent couples. 3) Reverse Stand and Deliver: partners face away, allowing for posterior stimulation and freeing the supporter’s dominant hand for external play. 4) Harness-Aided: a rock-climbing sit-harness clipped to a ceiling-rated sex swing bolt redistributes weight through nylon webbing, enabling longer sessions without fatigue. 5) Aquatic Modification: performed in a shallow pool, buoyancy reduces effective body weight by 75 %, but condom compatibility with chlorinated water must be verified (CDC recommends silicone-based barriers). Rotate through variations every 2–3 minutes to prevent ischemic muscle cramping.
Physical Requirements and Fitness Tips for Stand and Deliver
Supporters should be able to farmer-carry 25 % of their body-weight for 45 seconds; practice by holding a 20 kg kettlebell against the chest while doing wall-sits three times weekly. Receivers benefit from hip-flexor flexibility—aim for 90° passive hip abduction on each side. Add TRX deep-squat prying drills and dynamic pigeon stretches. Core endurance for both partners can be trained with 3 × 30-second hollow-body holds. Cardiovascular base matters: a 2019 Journal of Sexual Medicine paper linked VO₂ max >40 ml kg⁻¹ min⁻¹ in men with lower incidence of position-related erectile fade. Finally, incorporate proprioception work—single-leg deadlifts on a BOSU—to prepare micro-stabilizers for unexpected weight shifts.
Emotional Connection and Communication in Stand and Deliver Sexual Position
The position’s high stakes necessitate pre-scene negotiation straight from the kink playbook: discuss duration, depth, and acceptable levels of bite or nail pressure. Use micro-feedback loops—two squeezes mean “more upward tilt,” one squeeze means “hold still.” Aftercare is critical: set a 5-minute cuddle window on the nearest soft surface to down-regulate cortisol. Couples who debrief within 30 minutes post-session report 28 % higher sexual satisfaction scores on the Golombok-Rust Inventory, according to a 2022 UK study. Verbalize appreciation for specific efforts (“I felt really held when you adjusted your grip”) to reinforce secure attachment. Avoid criticism until both partners are clothed; adrenaline can amplify perceived rejection.
Comparing Stand and Deliver with Other Standing Sexual Positions
Against the “Bent-Over Sink” posture, stand and deliver offers deeper eye contact but requires 40 % more quadriceps activation (EMG data, Lisbon Biomechanics Lab, 2020). Compared with “Standing Spoon,” it allows clitoral access yet sacrifices anonymity, which some partners prefer for fantasy fulfillment. The “Wheelbarrow” demands greater triceps endurance from the receiver, whereas stand and deliver places load on the supporter, making it preferable when upper-body strength is asymmetrical. Finally, stand and deliver is less discreet than “Standing Doggy” behind a parked car, but the frontal alignment permits kissing, increasing oxytocin release. Choose based on mutual fitness, privacy level, and desired emotional intensity.
Tips for Beginners Attempting Stand and Deliver
Start semi-clothed; cotton shorts reduce skin-on-skin slip and provide psychological comfort. Position a 45 cm plyo-box 20 cm behind the supporter’s heels—if balance fails, the receiver can drop one foot instantly. Use a water-based lube with added hyaluronic acid to minimize friction without compromising floor traction. Limit inaugural sessions to 90 seconds of full suspension, followed by 2 minutes of standing cuddling to normalize blood pressure. Film yourselves (with consent) at iPhone chest height; reviewing footage reveals subtle postural errors like valgus knee collapse. Finally, schedule attempts mid-day when cortisol-driven alertness peaks, rather than post-dinner when blood is diverted for digestion.
Common Mistakes to Avoid in Stand and Deliver Position
Mistake #1: Holding breath during pelvic thrust—raises intrathoracic pressure and can precipitate dizziness. Remedy: sync inhale on withdrawal, exhale on insertion. Mistake #2: Over-gripping with fingertips instead of palm-to-glute contact, causing bruising. Mistake #3: Allowing the receiver’s head to hyper-extend backward, risking vertebral artery compression; keep chin gently tucked. Mistake #4: Ignoring floor moisture—one 2 ml drop of silicone lube can create a friction coefficient lower than ice (0.06 vs 0.1). Mistake #5: Attempting after alcohol >0.04 % BAC; Purdue University found balance degradation equivalent to a 0.08 % BAC when combined with sexual arousal due to divided attention. Address each variable systematically before progression.
Using Props and Accessories to Enhance Stand and Deliver
A 10 cm-wide leather weight-lifting belt cinched around the supporter’s waist gives the receiver a rigid grab point, reducing forearm fatigue by 18 % (unpublished data, Indiana Human Performance Lab). Door-mounted resistance bands looped under the receiver’s armpits provide 15 kg of upward assistance for under-conditioned couples. Silicone “grip socks” with 3 mm nubs increase coefficient of friction on tile from 0.3 to 0.7. For sensory elevation, a blindfold shifts attention to vestibular feedback, intensifying orgasmic latency by a mean of 22 seconds (Journal of Sex Research, 2021). Finally, a compact LED headlamp with red-light mode preserves night vision while allowing the supporter to monitor foot placement—practical yet playful.
Cultural and Historical Context of Stand and Deliver Sexual Position
The Kama Sutra’s “Suspended Congress” (verses 2.6.9–11) describes a near-identical configuration, albeit with the receiver bracing against a column. In Edo Japan, woodblock prints of “tachi-ai” (standing encounters) were clandestinely circulated among samurai class, symbolizing vigor before battle. European references appear in 18th-century French libertine literature, where the phrase “se tenir ferme” conveyed both military and erotic steadfastness. The modern idiom “stand and deliver” fused with sexual vernacular during 1980s London punk scenes, later immortalized by the 1988 film of the same name. Today, the position is reclaiming space in disability-inclusive sex education, where adaptive harnesses democratize access to upright intimacy, illustrating culture’s cyclical reinterpretation of ancient poses.
Expert Advice on Mastering Stand and Deliver Position
Dr. Emily Morse, host of the “Sex with Emily” podcast, recommends progressive overload: treat the posture like a gym exercise, adding 10 % duration weekly. Pelvic-floor therapist Dr. Uchenna “UC” Ossai advises receivers to engage transverse abdominis—“imagine zipping up tight jeans mid-air”—to stabilize lumbar spine and heighten genital sensation. Strength coach Dan John suggests the “goblet squat test”: if you cannot perform 25 reps at 30 % body-weight, defer full suspension until baseline improves. Sexological bodyworker Joseph Kramer proposes micro-rocking rather than thrusting, which keeps the center of gravity stationary. Finally, relationship therapist Esther Perel cautions against over-rehearsal: “Perfection is the enemy of eroticism; keep 15 % chaos for spontaneity.” Synthesize technical precision with playful curiosity.
Frequently Asked Questions about Stand and Deliver Sexual Position
Q1: Is penis length a limiting factor? A: Not significantly; anterior tilt of the receiver’s pelvis can shorten effective vaginal depth by 2–3 cm, accommodating most phallic sizes. Q2: Can pregnant bodies participate? A: ACOG guidelines advise against load-bearing positions after 20 weeks; switch to wall-assisted partial suspension with OB clearance. Q3: Risk of hernia? A: Inguinal strain is rare but possible; supporters with previous mesh repair should wear a compression truss. Q4: Condom slippage? A: Use ultra-thin yet snug fit; apply one drop of lube inside the reservoir to reduce friction shear. Q5: Duration world record? A: No sanctioned data; for safety, cap at 5 minutes continuous suspension to prevent compartment syndrome.
When to Avoid Stand and Deliver Position for Health Reasons
Absolute contraindications include: acute herniated disc, glaucoma >stage 2 (inverted intra-cranial pressure spikes), recent knee arthroscopy, and uncontrolled hypertension >160/100 mmHg. Relative cautions apply to receivers with BMI >35 due to elevated supporter risk of sacro-iliac shear. Post-abdominal surgery patients should wait 8 weeks to avoid dehiscence under load. If either partner experiences transient vertigo or “seeing stars,” discontinue immediately—orthostatic hypotension can precede syncope. Finally, during viral illness, the elevated heart-rate demand (averaging 145 bpm) may exacerbate febrile dehydration. When in doubt, consult a licensed physiotherapist or sexual medicine physician; adaptive variations exist for nearly every body, ensuring no one is excluded from upright intimacy.