Introduction to Positions for First Time Anal
Anal play can feel intimidating when you have zero experience, yet the right position lowers both physical risk and emotional anxiety. In Western sex-education circles, experts repeatedly stress that “position is protection”: the angle you choose directly affects how much control the receiving partner retains over depth, speed, and the all-important pause button. This guide starts from the ground up, assuming no prior knowledge and prioritizing consent, lubrication, and gradual progression. By framing positions as tools for communication rather than porn-style acrobatics, first-timers can replace fear with curiosity and discomfort with discoverable pleasure.
Why Positions for First Time Anal Are Essential
According to the American College of Obstetricians and Gynecologists, most anal injuries among novices stem from “excessive force in an angle that straightens the recto-anal junction.” In plain language, the wrong tilt plus too much enthusiasm equals micro-tears. A well-chosen beginner position keeps the natural curve of the rectum intact, lets the external sphincter relax, and gives the receptive partner an instant exit strategy. Beyond anatomy, positions set the emotional tone: face-to-face options foster eye-contact reassurance, while side-lying variants reduce performance pressure. In short, your position choice is the difference between a controlled experiment and an avoidable trip to urgent care.
Top Recommended Positions for First Time Anal
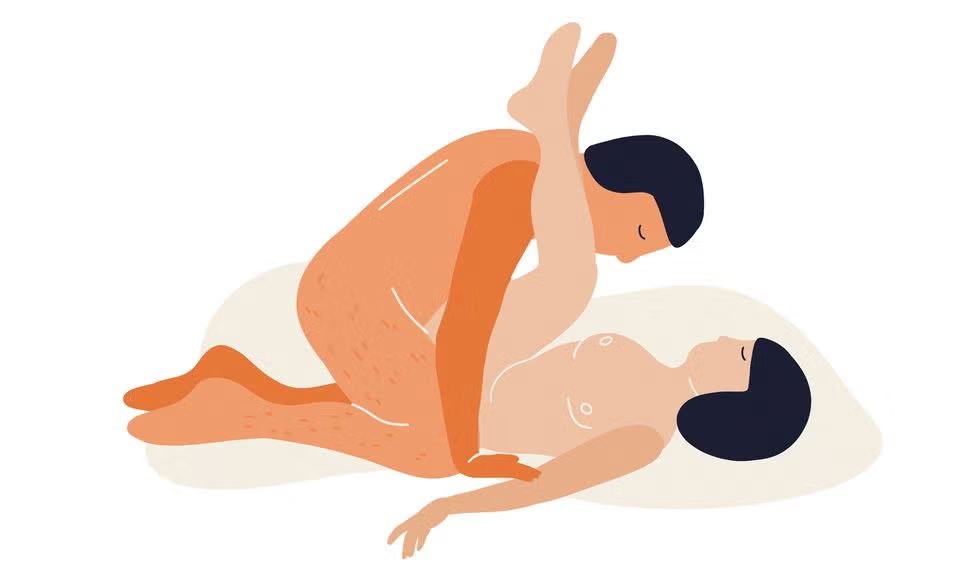
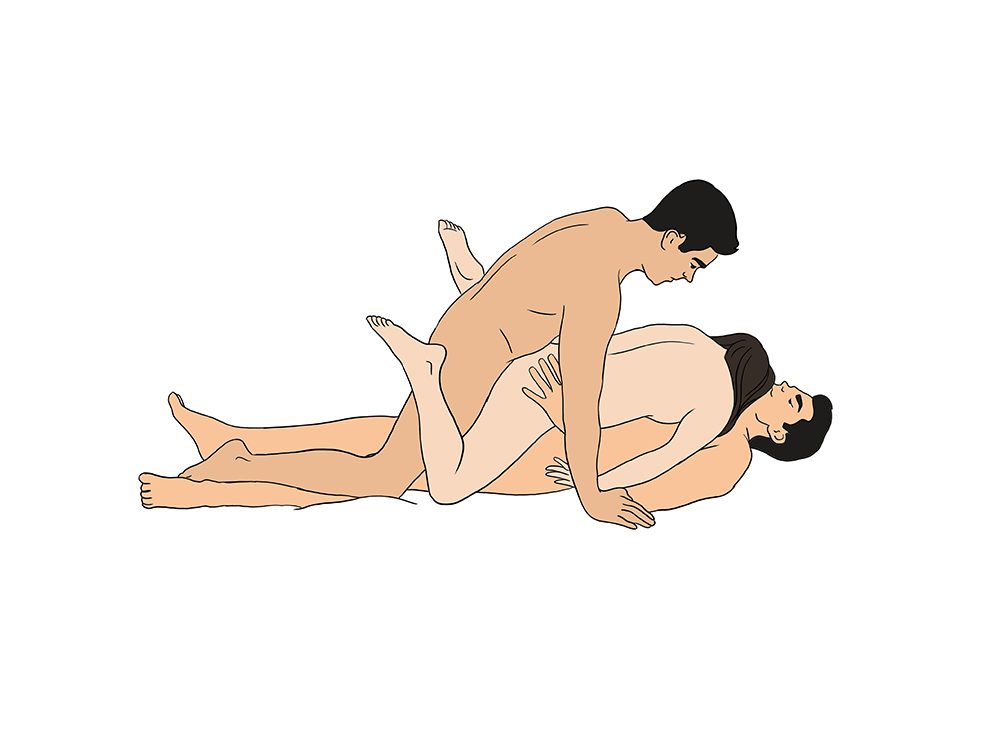
Three configurations consistently top the “safe start” lists compiled by Planned Parenthood and the UK’s NHS: (1) Spooning—both partners lie on their left side, knees bent; penetration is shallow and halted easily. (2) Modified missionary—receiver on back, receptive leg bent toward chest, giver kneeling; eye contact plus hand access for clitoral or penile stimulation. (3) Receiver-on-top straddle—giver lies flat, receiver lowers at their own pace; gravity becomes a built-in speed limit. Each option lets the receptive partner control depth with hip motion alone, no safe-word gymnastics required.
Safety Guidelines for Positions for First Time Anal
Before any position is attempted, three non-negotiables must be in place: consent reaffirmed, a silicone-based lubricant within reach, and a pre-agreed pause signal such as three quick taps. The Mayo Clinic warns that “numbing creams mask pain, the body’s early warning system,” so skip them. Trim nails, remove rings, and consider a condom-compatible glove for smoother entry. Keep baby wipes and a towel on the bed to avoid distraction spills, and never switch from anal to vaginal penetration without changing protection. Finally, plan aftercare: a warm blanket, hydration, and a two-minute check-in reduce post-scene drop.
How to Choose Positions for First Time Anal
Selection boils down to three personal variables: body mobility, prior pelvic-floor tone, and anxiety level. If hamstrings are tight or knees protest, skip doggy variations that require prolonged kneeling. Those with IBS or hemorrhoid history often find side-lying minimizes rectal pressure. Couples who process intimacy verbally should default to face-to-face poses; if embarrassment runs high, start in the dark with spooning. Test each candidate clothed first—mimic the hip angles on the living-room floor—to spot logistical red flags before anyone is emotionally exposed. When in doubt, the receiver’s comfort veto overrides every other consideration.
Preparation Steps: Lubrication and Relaxation
The anus does not self-lubricate, and micro-tears can facilitate STI transmission, so generous lube is medically advised. Choose a long-lasting silicone formula—Uberlube and Pjur Original are both condom-safe and glycerin-free, reducing yeast-risk for adjacent vaginal tissue. Warm the bottle in your palm first; cold shock triggers reflex tightening. Spend at least five minutes on external massage: circular pressure with a well-lubed finger around the outer sphincter teaches the muscle to yield without pain. Pair this with slow diaphragmatic breathing; a 2020 Journal of Sexual Medicine study found four-count inhales lowered pelvic-floor tension by 18 %, making penetration measurably easier.
Communication and Consent in Anal Play
Western sex therapists frame consent as an ongoing conversation, not a one-time checkbox. Use the “traffic-light” system: green for keep going, yellow for pause or adjust, red for full stop. Negotiate while horizontal clothes are still on; arousal clouds judgment and can inflate confidence beyond physical readiness. Discuss prior anal experience, IBS flare-ups, or hemorrhoid history—these disclosures are as vital as STI status. Agree that either partner can downgrade the plan to external rimming only; preserving the option to abort protects trust and often leads to a second, more relaxed attempt within the same week.
Missionary Position for Beginners
Classic missionary—receiver on back, a pillow under hips, knees toward chest—offers three beginner advantages: eye contact for real-time feedback, free hands for additional stimulation that distracts from initial stretch, and easy access for the giver to align with the receiver’s natural curve. Start with the giver resting the tip against the anus while the receiver bears down slightly on the exhale; no thrusting until the receiver nods. A folded towel under the sacrum prevents lube from pooling awkwardly. If the receiver’s thighs fatigue, resting calves over the giver’s shoulders converts the pose to a semi-doggy hybrid without relocation.
Doggy Style Position: Pros and Cons
Doggy grants the giver visual excitement and the receiver a sense of anonymity that can ease embarrassment, but it also allows the deepest penetration—risky for a virgin canal. To mitigate, receiver lowers chest to mattress, arching the lower back only mildly; this shortens the rectum and keeps the angle shallow. Place a firm pillow under the receiver’s hips to prevent collapse. The giver must initiate with shallow rocking, not thrusting, and keep one hand on the receiver’s hip as a tactile speed gauge. Because depth control is harder here, reserve doggy for attempt number two or three, after both partners have calibrated in a more restrictive pose.
Side-Lying Position for Comfort
Spooning is the gold standard for anyone with chronic lower-back pain, limited flexibility, or anxiety about mess. Both partners lie on their left side (the rectum straightens slightly on this side), knees bent 90 degrees. The receiver can clamp upper legs shut, creating an automatic gate that limits depth. The giver’s hands remain free to cradle the receiver’s chest, reinforcing security. A 2019 survey by the Kinsey Institute found side-lying scored highest for “comfort” and “control” among first-time anal receivers, with 78 % reporting zero pain when adequate lube was used. Bonus: the pose transitions seamlessly to sleep if both decide to stop.
Pain Management Techniques
Discomfort is usually a signal, not a sentence. First, differentiate between stretch pressure (normal) and sharp sting (halt immediately). Counter the former by syncing penetration with a voluntary push-down motion—mimicking a bowel movement—which opens the external sphincter reflexively. Adding clitoral or penile stimulation floods the body with arousal-induced endorphins that raise pain threshold by up to 40 %, according to a 2021 Rutgers University fMRI study. If burning persists, withdraw, add more lube, and downgrade to a smaller toy or finger for incremental desensitization. Never use numbing agents; they delay healing and obscure serious warning signs.
Aftercare and Hygiene Tips
Post-play, the rectal lining remains delicate for roughly 30 minutes. Cleanse externally with warm water only—soap disrupts mucosal pH. Offer the receiver a chamomile tea or a small sugary snack to counter vasovagal light-headedness. Inspect for bright-red spotting; a few drops are common, but steady bleeding warrants medical review. Store silicone toys in separate lint-free bags to prevent bacterial cross-contact, and launder towels on hot with fragrance-free detergent. Schedule a next-day text check-in; the “drop” phenomenon (emotional crash) can surface 12–24 hours later, and reassurance cements trust for future exploration.
Common Mistakes to Avoid
Porn scripts mislead: skipping warm-up, using saliva as lube, or jumping straight to penile penetration are the trifecta of first-time failure. Equally risky is the “just relax” command—without tactile guidance, the receiver tenses more. Avoid silicone toys with silicone lube; the chemical reaction creates a sticky surface that harbors bacteria. Double-dipping from anus to vagina is a UTI guarantee. Finally, don’t equate silence with consent; positional discomfort can freeze the receiver into non-responsiveness. Set an explicit verbal or tap-out safe word and honor it instantly, even if orgasm feels seconds away.
Psychological Readiness for First Time
Anxiety activates the sympathetic nervous system, which clamps the internal anal sphincter involuntarily. Cognitive-behavioral sex therapists recommend a “graded exposure” diary: rate anxiety 1–10 for each incremental step—talking, external touching, shallow insertion, full penetration—then repeat until the rating drops below 3. Visualization also works; spend five minutes nightly imagining the chosen position unfolding smoothly. If either partner carries prior trauma, consult a certified sex therapist (AASECT directory) before attempting penetration. Remember, readiness is a state, not a date; pushing through mental resistance converts curiosity into aversion and can stall anal exploration for years.
Additional Resources and Support
For evidence-based tutorials, visit Planned Parenthood’s “Anal Sex” hub and the American Sexual Health Association’s free PDF guide. Books: “Anal Pleasure & Health” by Jack Morin (widely cited by clinicians) and “The Ultimate Guide to Anal Sex for Women” by Tristan Taormino. Podcasts: “Sex with Emily” episodes 987 and 1012 feature urologists discussing pain-free mechanics. If cost is a barrier, the Trevor Project and Scarleteen offer free, LGBTQ-inclusive chat lines. Finally, should pain or bleeding persist beyond 24 hours, seek evaluation at a sexual health clinic—most municipal clinics provide sliding-scale care, ensuring your first exploration remains a memory, not a medical crisis.